

Safety and efficacy following 10-years of overnight orthokeratology for myopia control.
Abstract
PURPOSE: To compare rates of myopia progression and adverse events between orthokeratology (OK) and soft contact lens (SCL) wearers over a 10-year period in schoolchildren.
METHODS: Medical records of consecutive patients (≤16 years of age at baseline) who started OK for myopia correction and continued the treatment for 10 years were retrospectively reviewed. For the control group, patients who started using soft contact lenses (SCLs) for myopia correction and continued to use them for 10 years were also reviewed. Clinical data, including sex, age, manifest refraction, visual acuity, prescription lens power, and adverse events during the 10-year period, were recorded. Estimated myopia progression was calculated as the sum of ‘changes in prescription lens power during 10 years’ and ‘residual refractive errors at the 10-year visit,’ and was compared between groups. We also compared the incidence of adverse events between groups over the 10-year study period.
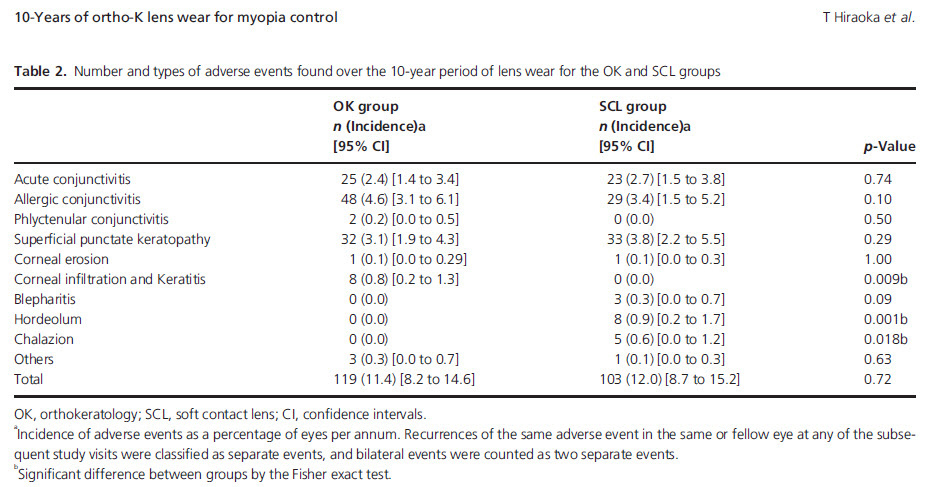
RESULTS: A total of 104 eyes of 53 patients who underwent OK treatment and 78 eyes of 39 patients who wore SCLs fulfilled the criteria. The estimated myopia progression over the 10-year period found in the OK and SCL groups were -1.26 ± 0.98 and -1.79 ± 1.24 days, respectively; this difference was statistically significant (p = 0.001). Additionally, lower myopia progression was found in the OK in comparison to the SCL group at all baseline ages (p = 0.003 to p = 0.049) except at 16 years old (p = 0.41). No significant difference was found in the number of adverse events found between the OK (119) and SCL (103) groups (p = 0.72).
CONCLUSIONS: The results of this study supports the long-term efficacy and safety of OK lens wear in reducing myopia progression in schoolchildren.
OSO Comment: This paper is the first to retrospectively look at the efficacy and safety over a period of a decade compared to soft contact lenses. Unfortunately their method for evaluating myopia progression in the orthokeratology wearers was the use the change in base-curve of the OK lens and the residual refraction, both of which are not very precise metrics in an ortho-k wearer.
Their data confirmed that patients who became myopic younger progress more with both ortho-k and SCLS, although estimated progression with ortho-k wear is slower than SCLs in all ages except 16yo.
Pleasingly no significant difference in adverse events were found between the groups. Interestingly there was a much higher numbers of blepharitis, hordeolum and chalazion in the SCL wearers (16 vs 0 in ortho-k wearer), whereas the ortho-k patients had more corneal events (8 vs 0 in SCL wearers). There were no infective keratitis in either groups over the 10 year period.
This data is useful to show that overall ortho-k is as safe an option as soft contact lens wear over the long period we expect our young patients to be at risk of myopia progression.
Author: Alex Petty (Orthokeratology Society of Oceania)
RESULTS: A total of 104 eyes of 53 patients who underwent OK treatment and 78 eyes of 39 patients who wore SCLs fulfilled the criteria. The estimated myopia progression over the 10-year period found in the OK and SCL groups were -1.26 ± 0.98 and -1.79 ± 1.24 days, respectively; this difference was statistically significant (p = 0.001). Additionally, lower myopia progression was found in the OK in comparison to the SCL group at all baseline ages (p = 0.003 to p = 0.049) except at 16 years old (p = 0.41). No significant difference was found in the number of adverse events found between the OK (119) and SCL (103) groups (p = 0.72).
CONCLUSIONS: The results of this study supports the long-term efficacy and safety of OK lens wear in reducing myopia progression in schoolchildren.
OSO Comment: This paper is the first to retrospectively look at the efficacy and safety over a period of a decade compared to soft contact lenses. Unfortunately their method for evaluating myopia progression in the orthokeratology wearers was the use the change in base-curve of the OK lens and the residual refraction, both of which are not very precise metrics in an ortho-k wearer.
Their data confirmed that patients who became myopic younger progress more with both ortho-k and SCLS, although estimated progression with ortho-k wear is slower than SCLs in all ages except 16yo.
Pleasingly no significant difference in adverse events were found between the groups. Interestingly there was a much higher numbers of blepharitis, hordeolum and chalazion in the SCL wearers (16 vs 0 in ortho-k wearer), whereas the ortho-k patients had more corneal events (8 vs 0 in SCL wearers). There were no infective keratitis in either groups over the 10 year period.
This data is useful to show that overall ortho-k is as safe an option as soft contact lens wear over the long period we expect our young patients to be at risk of myopia progression.
Author: Alex Petty (Orthokeratology Society of Oceania)